Archive for the ‘renal’ Category
Wilm’s Tumor
- Age: 80% <6yo; most common abdominal neoplasm 1-8 yo.
- Appearance: solid mass in kidney (claw sign), pushing away vessels, not crossing mid-line
- IVC and renal vein thrombosis
- Mets to lung, liver, brain, bone
- Staging
- I = confined to kidney
- II = local extension to perinephric space
- III = lymph nodes
- IV = distant mets
- V = bilateral renal
- DDx: neuroblastoma (crosses mid-line, encases vessels, calcify), multilocular cystic nephroma, sarcoma, RCC, nephroblastomatosis, mesoblastic nephroma, AML, renal medullary carcinoma
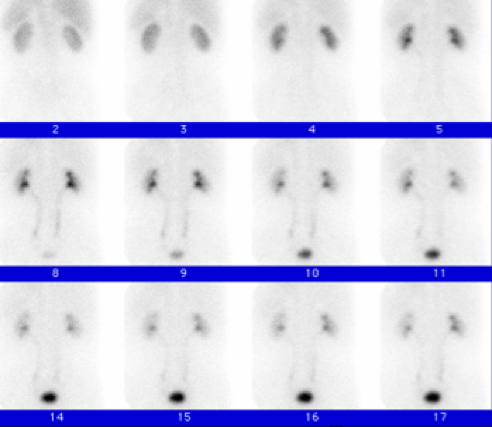
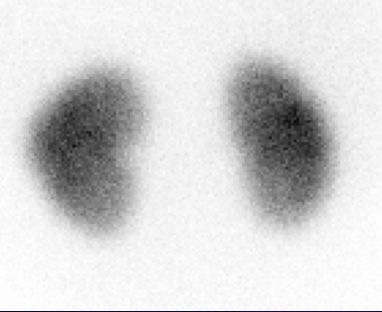
Renal Scintigraphy
- Perfusion/Obstruction
- normal uptake 50/50 L and R kidney; >60/40 is abnormal
- normal peak < 5 minutes
- normal residual coritcal activiy < 0.3
- Lasix
- increases urine output
- inject 15 min before MAG3/DTPA
- no washout after Lasix = obstruction
- normal T1/2 = < 10 min
- obstructed T1/2 = >20 min
- Captopril
- evaluate renal artery (renal artery stenosis, ischemia, renovascular hypertension)
- baseline scan, captopril scan, post scan
- high prob RVH = marked captopril induced changed
- for UTI or pyelonephritis, congenital malformation
- cold spots: pyelonnephritis, tumors, cyts, hydronephrosis, trauma, infarct
- UTI, VUR
- sulfur colloid, DTPA, MAG-3
- fill bladder until reverse flow
Source: ppt
Pediatric Renal Tumors
- Wilm’s tumor
- nephroblastomatosis
- Clear cell sarcoma
- Rhabdoid tumor
- Hamartoma
- Angiomyolipoma
- Ossifying Renal Tumor of Infancy
- Metanrphric Adenoma
- Adjacent Neuroblastoma from adrenal gland

Decreased renal echogenicity
- Acute pyelonephritis
- Renal vein thrombosis
- Acute glomerulonephritis
- Lupus nephritis
- Lymphoma
Increased renal echogenicity
Cortical only:
- Acute/Chronic Glomerulonephritis
- Nephrosclerosis
- Acute tubular necrosis
Medullary only:
- Medullary nephrocalcinosis
- Renal pyramidal fibrosis
Cortical and Medullary:
- Chronic Plyeonephritis
- Chronic Glomerulonephritis
Patchy:
- Infection
- Scarring
- Renal Vein thrombosis
Big Kidneys Differential
Unilateral
- Compensatory hypertrophy
- Pyelonephritis
- Duplex kidney
- Renal Vein Thrombosis
- Hydronephrosis
- Acute renal infarct
Bilateral
- Unilateral cases as above
- AD PCKD
- AR PCKD
- Glomerulonephritis
- Acute tubular necrosis
- Diabetic nephropathy
In Kids:
- Nephroblastomatosis
- Nephrotic Syndrome
- Polycystic Kidney disease
- Glycogen Storage
- Lymphoma/Leukemia
Renal Laceration Grading
Grade 1
- hematuria, normal imaging
- contusion
- nonexpanding subcapsular hematomas
Grade 2
- nonexpanding perinephric hematoma confined to the retroperitoneum
- laceration <1cm deep, collecting system not involved
Grade 3
- laceration >1cm, collecting system not involved
Grade 4
- laceration extending to collecting system
- involve main renal artery or vein
- segmental infarctions without associated lacerations
- expanding subcapsular hematomas compressing kidney
Grade 5
- shattered or devascularized kidney
- ureteropelvic avulsions
- complete laceration or thrombus or main RA or V
Abnormal Renal Vasculature
- multiple renal arties is common, 25% of population
- second, diminutive artery supplying lower pole
- supernumerary veins, less common than arteries
- left is retroaortic
- significant for preop planning
Fibromuscular Dysplasia

- Medium to large artery vasculitis
- Most commonly affects renal arteries
- 15-20 yo females with refractory HTN
- MRA or arteriography: stenosis and post-stenotic dilitation, string or beads appearance.
- all layers affected: intima, media, adventitia
Grades of Ureteral Reflux
| Grade | Findings |
| I | Reflux confined to ureter only |
| II | Reflux to the level of the intrarenal collecting system without dilatation |
| III | Grade II + mild or moderate dilatation of the ureter or renal pelvis, but no or only slight forniceal blunting |
| IV | Grade II + calyceal dilatation and obliteration of the sharp angle of the fornices, but maintainance of the papillary impressions |
| V | Gross dilatation and tortuosity of the ureter; gross dilatation of the renal pelvis and calices; papillary impressions are no longer visible |
Grades I-III: Typically resolve as the child grows
Grades IV-V: Typically require surgery to correct
http://www.auntminnie.com/index.asp?sec=ref&sub=ncm&pag=get&itemid=54506
Renal Function and Iodinated Contrast
- Hold metformin prior and 2 days after
- Hold diuretics 1 day prior
- hydrate with IV normal saline
- Mucomyst 1200mg IV prior to CT or 600mg PO BID before and after scan, or…
- Bicarb 3ml/kg/hr x 1hr prior and 1ml/kg/hr x 6hrs afterwards (mix 3 amps in 1L of D5 water, bolus 500cc prior to ct, then 100cc per hour until its gone)
Cr less than 1.4 = full dose contrast
Cr 1.5-2.0 = do above.
Cr greater than 2.0 = consider alternative test
Bosniak CT Classification of Cystic Masses
I = simple cyst; nonoperative
II = septated, minimal calcium, nonenhancing high-density cysts, infected cysts; nonoperative
III = multiloculated, hemorrhagic, dense calcification, non-enhancing solid component; renal-sparing component
IV = marginal irregularity, enhancing solid component; Radical nephrectomy
Renal Masses
see differentials for solid and cystic renal masses.
Solitary Expansile Masses
- Cystic Lesions
- Renal Cell Carcinoma
- Oncocytoma
- Multilocular Cystic Nephroma
- Renal Abscess
- Focal XGP
- Renal Metastasis
- Angiomyolipoma
Multiple Expansile Masses
- Polycystic Kidney Disease
- Medullary Cystic Disease
- Juvenile Nephronophthisis
- von Hippel-Lindau Disease
- Acquired Cystic Disease of Dialysis
- multiple RCC (2% of RCC)
- metastasis (colon)
- lymphoma
- multiple abscesses
- multiple oncocytomas (central stellate scar)
Geographic Infiltrating Masses
- Transitional Cell Carcinoma
- Squamous Cell Carcinoma
- Renal Medullary Carcinoma (invade renal sinus, African Americans)
- Collecting Duct Carcinomas
- Lymphoma and Metastasis
- Pyelonephritis
- renal tuberculosis
- XGP
- Renal Infarction
Subcapsular Renal Hematoma
 subcapsular mass with effacement of renal parenchyma
subcapsular mass with effacement of renal parenchyma- resorbed and calcifies with time, forms pseudocapsule
- complication: Page Kidney (ischemia, HTN, renin release)

http://brighamrad.harvard.edu/Cases/bwh/hcache/127/full.html
Retroperitoneal Hemorrhage
Spontaneous: Sudden onset flank pain. Surgery is indicated if etiology not determined by imaging. Do f/u CT in 3-6 month if source of bleed indeterminate.
- Renal tumor (malignant and benign)
- Vascular: ruptured renal artery aneurysm, vasculitis, AVM, segmental renal infarction
- Inflammation/Infection: abscess, nephritis
- Coagulopathy
- Adrenal Tumor: pheochromocytoma, pseudocyst, leylolipoma, hemangioma, adenoma, met
Trauma – 3 retroperitoneal zones:

Compartments and Planes:


Resistive Index on Renal Doppler
Normal RI <0.70.
- renal medical disease (vascular/tubulointerstitial process >> glomerular disease)
- significant systemic hypotension
- markedly decreased HR
- perinephric or subcapsular fluid collections
- neonate and infants
Tuberous Sclerosis
- Autosomal dominant neuroectodermal disorder characterized by multifocal systemic hamartomas and malformation
- 30% dead by age 5, 75% dead by age 20
- affects CNS, kidney, lung, skin, heart
- Triad: zits, fits, nitwits (facial angiofibroma, epileptic seizures, MR)
- chromosome 9 and 16
- Diagnostic criteria: 2 major or 1 major + 2 minor
Major
- cortical/subcortical involvement
- subependymal giant cell astrocytoma
- cardiac rhabdomyoma
- facial angiofibroma
- retinal hamartomas
- renal angiomyolipoma
- Shagreen patches
- Ash-leaf spots
- Lymphanioleiomyomatosis
Minor
- gingival fibroma
- dental pits
- hamartomatous rectal polyps
- renal cysts
- cerebral WM migration lines
- Confetti skin lesions
- bone cysts
CNS involement
- subependymal hamartomas
- giant cell astrocytoma
- cortical/subcortical tubers
- heterotopic gray matter islands in white matter
Skin involvement
- facial angiofibromas
- Shagreen rouch skin patches = “pigskin”
- ash leaf patches
- ungual fibromas
- cafe-au-lait spots
Occular involvement
- phakoma
Renal Involvement
- angiomyolipoma
- multiple cysts
- renal cell carcinoma
Other
- lung: progressive respiratory insufficiency
- heart: cardiomyopathy, rhabdomyoma of ventricle or atrium, aortic aneurysm
- bone: bone islands, periosteal thickening, bone cysts
- adenomas of liver, pancreas, spleen
- vascular: aortic aneurysms







{kind=link}
{kind=link}
{kind=link}